Essential Tremor
A common movement disorder that causes rhythmic shaking — most often in the hands during everyday activities. When medication isn't enough, advanced treatment options can help restore control and quality of life.
Very common condition
Affects hands, head, and voice. Many manage well with medication, but some need advanced treatment.
Three advanced options
Robotic DBS, MRI-guided focused ultrasound, and radiosurgical thalamotomy each offer distinct advantages.
Personalized to you
The best approach depends on your tremor pattern, goals, medical history, and anatomy.
What is essential tremor?
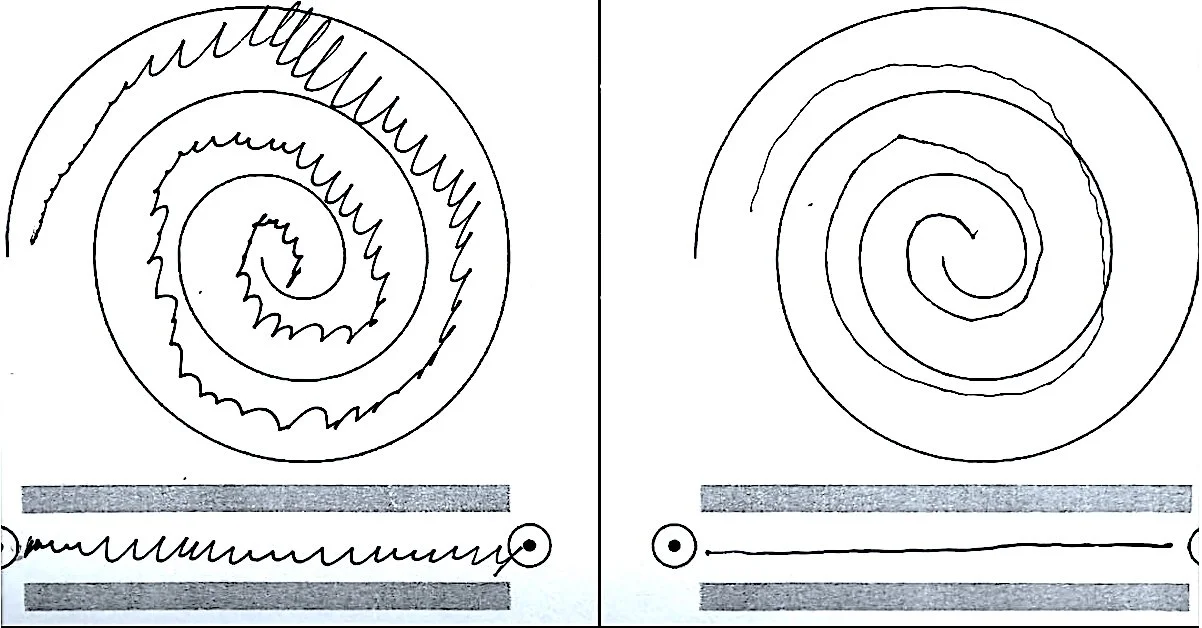
Essential tremor causes rhythmic, involuntary shaking — most often in the hands during action like writing, eating, or using tools. Unlike the tremor seen in Parkinson's disease, essential tremor typically occurs during movement rather than at rest.
Symptoms may progress over time and can affect your independence and quality of life. Many people respond well to medications such as propranolol or primidone, but when these aren't enough, procedure-based treatments can offer meaningful improvement.
Who may benefit from procedure-based treatment?
You may be a candidate if:
These criteria help us determine whether an advanced approach could help you.
- Your tremor is functionally disabling — daily activities like writing, eating, or drinking are significantly impacted despite trying medications (often propranolol and/or primidone).
- Your diagnosis is consistent with essential tremor or tremor-predominant Parkinson's disease, sometimes confirmed by a movement-disorder specialist evaluation.
- You can participate in follow-up care — programming visits for DBS, or monitoring after lesioning procedures.
Treatment Options
Each approach targets the same brain circuit but in a different way. Understanding the trade-offs can help you make the right decision for your situation.
Robotic DBS
Deep Brain Stimulation with robot-assisted precision
MRI-Guided Focused Ultrasound
Incisionless thalamotomy (MRgFUS)
GammaKnife Radiosurgical Thalamotomy
Precision radiation-based lesioning
Side-by-side comparison
A quick reference to help you compare the three approaches.
| Feature | Robotic DBS | MRgFUS | GammaKnife |
|---|---|---|---|
| Incision | Small surgical incisions | None | None |
| Implant | Electrodes + battery | None | None |
| Adjustable | ✓ Yes — can be tuned | ✗ Permanent lesion | ✗ Permanent lesion |
| Reversible | ✓ Can be turned off | ✗ Not reversible | ✗ Not reversible |
| Bilateral | Often both sides | Staged, selected patients | Staged, selected patients |
| Onset of effect | Weeks (after programming) | Often immediate | Weeks to months |
| Typical stay | 1–2 nights | Same day | Same day |
| Anesthesia | General or local + sedation | Local (awake) | None |
| Skull requirement | None specific | Adequate skull density/shape | None specific |
What to Expect
Here's an overview of the process, regardless of which treatment you and your doctor choose.
Before your procedure
Neurologic evaluation, brain MRI/CT planning, medication review, and a discussion of your goals — including which hand to prioritize, whether voice or head tremor is involved, and what matters most to you in daily life.
During
DBS: Surgery to place leads, then generator placement; programming begins weeks later.
MRgFUS: MRI-suite procedure (~2 hours), awake with real-time feedback, no incision.
Radiosurgery: Head frame placement, treatment delivery, typically outpatient.
After
DBS requires programming "fine-tuning" over multiple visits. Lesioning procedures (MRgFUS and radiosurgery) require monitoring for balance or sensory effects. Follow-up imaging and symptom tracking help ensure the best possible outcome.
Benefits and Risks
Potential Benefits
- Meaningful tremor reduction — usually above 80% improvement
- Improved ability to write, eat, drink, and use tools
- DBS offers adjustability and bilateral treatment option
- MRgFUS and radiosurgery avoid implants
Possible Risks
- Common: Temporary headache, nausea, transient balance or sensory symptoms (varies by procedure)
- Uncommon: Bleeding, stroke, infection (implant procedures), seizure, persistent neurologic effects, or delayed radiation injury
Patient FAQs
Will DBS stop my tremor completely?
Is focused ultrasound "safer" because it's incisionless?
How long does radiosurgery take to work?
Can I treat both sides?
Will I still need medications?
When to Seek Urgent Care
Call your care team right away — or go to the ER (or call 911) — for sudden weakness or numbness, a severe or worsening headache, confusion, seizure, fever, wound redness or drainage (DBS), or new trouble walking that is getting worse quickly.